WHAT IS CHOLESTEATOMA:
First I would like to explain what a cholesteatoma is and it’s complications.
It is a rare but serious disorder – the annual incidence of cholesteatoma is 3 per 100 000 in children and 9.2 per 100 000 in adults with a male predominance of 1.4:1.
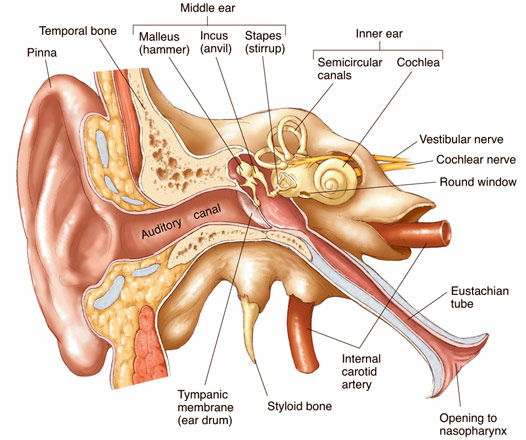
It is a benign cyst in the middle ear, behind the ear drum. Although cholesteatoma is not a tumour, it behaves like one. It can form due to a retraction pocket of the ear drum. This retraction pocket forms when the eustachian tube that normally drains the ear into the back part of the nasal cavity does not function well, and a vacuum develops behind the drum. This vacuum then starts to pull the eardrum inward, and if this process continues long enough, pockets or pouches can form from it. The outer layer of the ear drum is a very thin layer of skin. As this pocket or pouch continues to enlarge, the skin lining of the pocket has more difficulty getting rid of the dead skin, and therefore, it starts to accumulate. As it accumulates within the pouch, it can get infected or can start to erode some of the bony structures in the middle ear, such as the ossicles (the small bones conducting sound from the eardrum to the inner ear) or the bony structure (cochlea) that houses the inner ear or the bony covering of the facial nerve which can lead to paralysing of the face. Mastoiditis may occur with spread of the cholesteatoma infection into the mastoid bone (behind the outer ear). Severe vertigo may be present if the cholesteatoma begins to erode the semicircular canal of the inner ear. Cholesteatoma can even cause damage to blood vessels supplying brain structures. If the cholesteatoma is extensive, it can erode the bone between the middle ear and brain. Infection in the skin cyst may then spread to the brain cavity, causing meningitis. This infection can also spread into the cranium (intracranial abscess)
Another way in which a cholesteatoma can form is if there is a hole in the eardrum (perforation). This is particularly likely if the edge of the hole is in contact with the outer ear canal. The skin that lines the ear canal or the eardrum can then grow through the perforation into the middle ear and then the enlarging mass of skin can accumulate, creating the same problem mentioned above for a retraction pocket cholesteatoma. Lastly, it is also thought that chronic inflammation in the middle ear can lead to cholesteatoma. With chronic inflammation of any mucous membrane surface it can start to change into a lining more similar to skin. If this transformation becomes complete, then skin can replace areas of the normal mucous membrane behind the eardrum. Since the shedding skin is then trapped behind the eardrum, the skin continues to accumulate and can result in infection or destruction of middle ear structures.
SURGERY AND TREATMENT:
The problem with cholesteatoma, is that it’s usually not a one time thing. Just when you think it’s all over and you’ve had your surgery and ENT check ups, it comes back creeping and growing. Cholesteatoma can be a silent and relentless process for years before symptoms advance.
A good portion of my childhood consisted of A LOT of hospital and ENT visits. I was very much in and out of hospitals. I’ve had 4 surgeries in 3 different hospitals, surgeries that take hours to perform, and one conservative treatment. When I wasn’t at the hospital, I was getting regular suctions for my ear discharge and putting ear drops in my ear. Till this day, even if it’s been years since my last suction, I still have a very vivid memory of the pipes and sound of these suctions. Ear infections were just so common place for me. And when I wasn’t getting treatment, I was getting an audiometry, many of them. I can’t even begin to describe how much time I spent at the doctors office and hospitals. I have so much respect and admiration for what these doctors do, without them I wouldn’t be here today. Just the performance of the surgery, which were all done by professors, are extremely complicated surgeries. The same structures that are at risk from the disease are at risk from the operation to remove the cholesteatoma. And even with all the latest high powered microscopes, lasers and modern anaesthetics, mastoid surgery is very difficult. The margin of error in mastoid surgery is measured in fractions of a millimetre. Anatomy varies considerably, and a surgeon needs to practice on lots of bones before embarking on live patients. From a patients perspective, the fear before each surgery has been indescribable, you never get used to it, despite all the trust I have towards these excellent surgeons.
Before my first surgery in 1989, I had gone for months and months with a chronic infection. The stench of the infection was so bad, kids would bully me because of it. Unfortunately the ENT at the time had diagnosed my ear infection as a typical children ear infection. The diagnosis of cholesteatoma is sadly often delayed. Despite all the antibiotics, nothing was removing the infection until I was finally diagnosed with cholesteatoma. By the time I was diagnosed, the cholesteatoma had grown into the inner ear and caused permanent sensorineural hearing loss, which is damage to the cochlea or hearing nerve. The cholesteatoma had also caused conductive hearing loss, due to the damage of my ossicle bones. 3 years later I was operated again and a titanium implant was inserted to replace the damage to my ossicle bones (the photo is from my surgery in 2007 where a new implant was inserted due to the previous one fallen loose). The first operation was the longest operation, it lasted for several hours. The pain after the operation was excruciating. I would scream for hours in pain. Nurses would literally run back and forth, although there was nothing they could do as I was given max pain killers. Nurses would stand next to me while holding the pulp kidney dish until it was full from vomit, then hand me another one, and another one…. I was hospitalised for about a week. My experience is that operations were usually more dramatic as a child. The older I got, the less dramatic. The last operation was in 2007. Before the operation, I had agreed to have a full class of medical students to have a look in my ear. The operation went very well and was a big success. My eustachian tube was dilated for better drainage, the cholesteatoma was removed (all of it) and a new implant was inserted. I have not had an ear infection in almost 9 years! Unfortunately I do have a cranial vene that is defect due to the cholesteatoma. But so far no reoccurrences in almost 9 years (hopefully) and no more frequent visits to the ENT and hospitals, although check ups are life long. My last hearing test which was in april 2014, shows a mild hearing loss on my right ear (mild hearing loss have thresholds between 26 and 40 dB HL). My threshold in average is close to 40 db HL in my right ear, so it’s close to moderate hearing loss. I have especially difficulties with high frequencies, which means that it’s particularly difficult to hear consonants.
THE EFFECTS OF HEARING LOSS AND IT’S STIGMA:
This is the part where I want to talk about the effects hearing loss has had on me. Ah…the ear, such an incredible organ that we are still discovering, and that most people take for granted. Hearing is a lot more complicated than people assume. Unfortunately, there is not enough recognition given to hearing loss, which is why I decided to write this blog. Even if there is more awareness on the deaf and hearing loss, there are still too many misconceptions, prejudice and stigmas. Stigmas such as ‘’they are less intelligent’’, ‘’they only hear what they want to hear’’ and so on. Of course these are highly inaccurate.
You would be surprised how much brain energy I use just by listening and concentrating, to compensate for the hearing loss which can be exhausting. This can be embarrassing, because sometimes the subject is mentioned at a later point, but I don’t have a clue of what you are talking about. However, I can concentrate on reading for hours with hardly any breaks.
Also, my experience is that sometimes people get annoyed with having to repeat themselfs, so this is partially why I sometimes just give up. In the worst case scenario I’ve actually had someone try to convince me that there was ‘’another psychological reason’’ for my ‘’so called’’ hearing loss. Fortunately I’ve only experienced this once. But it’s a slap in the face, discrediting any hearing loss one may have. It’s extremely unpleasant. My hearing loss is not something I can just remote control and edit as I wish. I’ve also had a colleague take advantage of my hearing loss, knowing full well I would not be able to hear what she was saying. But these are fortunately rare cases.
I don’t do well with accents, mumbling, too much background noise, when people turn their backs, and when people talk too fast. Sometimes words even get mistaken for other words. Trying to put all the effort you can in trying to hear what is being said, can be very draining.
Also, because there is so much stigma on hearing loss, I’ve missed out in classes. Instead of insisting on sitting in front in order to hear better, I would hide my disability and sit further away. Hearing loss is tabu. On the other hand I believe that us with hearing loss are partially responsible for this stigma by not being more open about it. Unfortunately, it’s only recently that I have begun to tell people of my hearing loss, especially at work places. Besides the negatives, I’ve also had some very pleasant experiences where people have been very considerate of my hearing loss. Eg. I had a co-worker who would often remind me to sit close to the person who was giving the morning report. The reason why she’d have to remind me, is because it’s still deep engraved in me to hide that I have a disability. It’s a process hard to break.
At last, there are still prejudices such as people with hearing loss should just wear hearing aids. It is not that simple. Normal hearing aids can help, but the sound quality isn’t always great, and they often cause infection. Blocking the ear canal with a hearing aid mould makes it moist. This encourages germs. Many cholesteatoma patients find that they can’t wear hearing aids because they cause infection, with painful, discharging ears. They have to stop wearing the hearing aid, get treatment for the infection with microsuction and antibiotic / steroid ear drops, and are unable to hear properly for weeks. Once the infection clears up, they go back to wearing the hearing aid, then the whole miserable cycle repeats itself.
I believe that not being able to hear so well, has given me a huge appreciation for music. Listening to music and playing the piano is one of my absolute favourite hobbies. Rollerblading, which has to do with balance is also another one of my favourite hobbies. And I can only thank science and the excellent, wonderful doctors and surgeons for me to be able to enjoy these things and appreciate them.
I hope that this can give some in sight and awareness to what it is like dealing with hearing loss cholesteatoma.
If you would like to know more about cholesteatoma, this is an excellent and worthwhile article to read: http://entkent.com/cholesteatoma-and-mastoid-surgery/
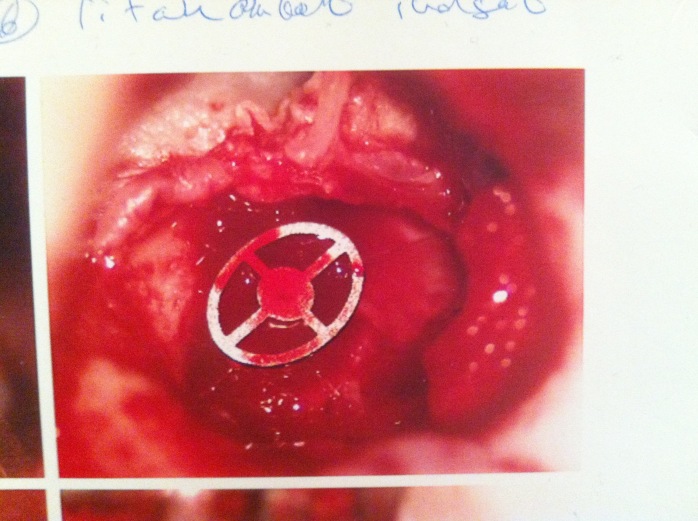
2007 titanium implant.